Iliotibial band: What is the function and how to manage discomfort?
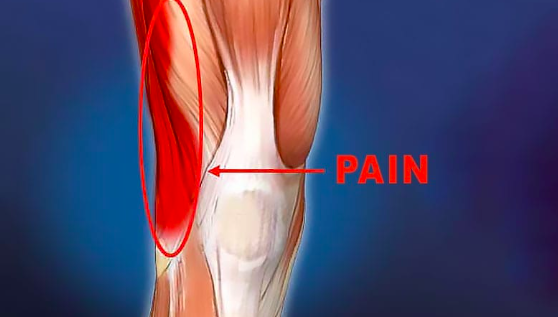
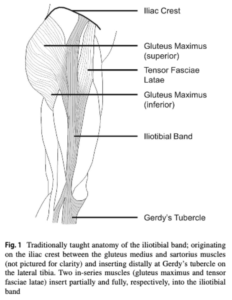
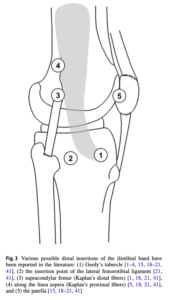
The iliotibial band (ITB) stands as a resilient and fibrous fascial tissue, stretching from the iliac crest to the lateral proximal tibia, intricately woven into human posture when standing.
Despite its pivotal role, the mechanical functions and foundational anatomy of the ITB still pose challenges for full understanding, fuelling ongoing research. Functionally, the ITB has a dual role in stabilising the hip and knee, especially in the frontal plane. Additionally, it’s thought to have potential involvement in storing elastic energy during walking.
However, this seemingly indispensable structure isn’t exempt from issues. Runners often grapple with ITB pain, with a prevalence ranging from 5% to 14% of all running-related injuries. This articles will discuss everything we know so far about the iliotibial band, its function and dysfunction, highlighting key diagnostic tests and the management of iliotibial band syndome.
It will highlight key information from the research study:
Hutchinson, L.A., Lichtwark, G.A., Willy, R.W. and Kelly, L.A., 2022. The iliotibial band: a complex structure with versatile functions. Sports Medicine, 52(5), pp.995-1008
Join our newsletter and fun infographics that analyse complex sports medicine ressearch
Anatomical variance
Human Uniqueness in the Iliotibial Band
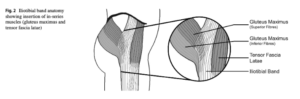
Human anatomy boasts evolutionary uniqueness, especially in the context of the ITB and associated muscles. One standout feature is the human gluteus maximus muscle, which surpasses its non-human primate counterparts in size. This size discrepancy isn’t just a quirk; it plays a pivotal role in enhancing trunk stabilisation, a key adaptation for human erect posture.
Unlike other primates, humans exhibit a structurally distinct ITB, setting them apart anatomically. The human ITB deviates from the fascia lata seen in other primate species, marking a unique evolutionary trajectory.
An additional anomaly lies in the location of the tensor fasciae latae (TFL) muscle in humans. Unlike other animals, the TFL in humans reaches the superior thigh, inserting into the femur near the greater trochanter.
The evolution from walking on all fours to just two is attributed to a combination of factors, including the well-developed gluteus maximus, a shift in pelvic position from horizontal to vertical, and the distinctive formation of the ITB.
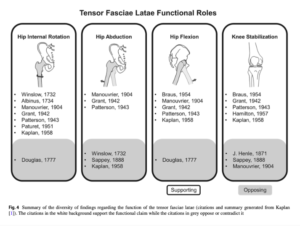
Tensor Fascia Latae Biomechanics
The consensus supports TFL’s involvement in hip internal rotation, hip flexion, and knee stabilisation, however its high electromyographic (EMG) activity during isolated abduction has fuelled debates surrounding its primary function.
Speculation regarding TFL’s potential role in hip abduction exists, but the prevailing view contends that any force it exerts at the knee is transmitted via the ITB, implying a stabilising role at the knee rather than an active contributor to joint movement.
Gottschalk et al.’s innovative concept positions the ITB as a “strut” during normal walking, providing frontal plane stabilisation for the hip. Recent research by Neumann delves into the theoretical potential actions of hip muscles, suggesting that TFL, with its frontal plane moment arm, may play a vital role in stabilising the pelvis in the frontal plane.
Notably, the mechanical role of TFL likely hinges on the posture of the ITB during force production, considering its double joint nature and shared insertion onto the ITB with the gluteus maximus, a muscle opposing hip flexion.
TFL’s biomechanics not only highlights the complexities within the hip musculature but also emphasises the interconnected nature of muscles and their roles in maintaining stability and orchestrating movement throughout the body.
The impact of ITB on compression forces
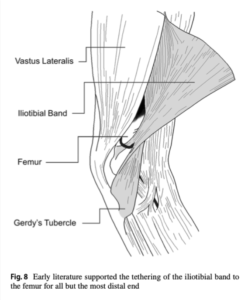
ITB’s resistance to external adduction type forces after direct impact and the knee compression force to the femur through ITB tensioning contribute significantly to achieving stability.
Magnetic resonance images provide a visual testament to the impact of ITB tensioning, showing compression in the tissues between the distal ITB and the lateral femoral epicondyle. This compression mechanism, integral to knee joint stability, demonstrates the interesting dynamics at play during movement.
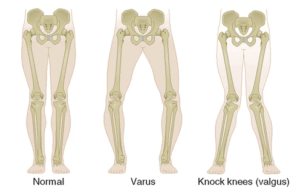
However, the delicate balance between stability and potential challenges comes to the forefront in discussions surrounding iliotibial band syndrome (ITBS). Current theories propose ITBS as a compression syndrome, suggesting that the enhanced knee joint stability provided by the ITB may, in some instances, lead to potentially unfavourable excessive compression. This is particularly notable in the presence of varus knee torques, where the forces on the knee are directed inward, potentially exacerbating compression-related issues.
In lab & out of lab material properties and elastic function
Material Properties of ITB & understanding how it affects biomechanics
The material behaviour of the ITB is pivotal to know if we want to understand the roles it plays in human movement and stability. Acting as a vital connection point for muscles, such as the gluteus maximus and TFL, to bones like the pelvis, femur, and tibia, the ITB suggests tendon-like material properties, contributing significantly to joint stability and potentially participating in elastic energy storage and release, just like the Achilles tendon.
While the general material properties of the ITB are well-documented, the overall mechanical behaviour of the entire structure remains somewhat blurred. Tensioning of ITB fibers during hip extension follows an anterior-to-posterior pattern, resulting in varied tension across different regions of the band based on movement patterns.
The transmission of forces within the ITB unfolds as a diverse process, influenced by the specific muscles generating forces.
You May Also Like
Graft rupture risk factors after ACL-Reconstruction
Delving into the complexities of ACL injuries, especially in athletes who have undergone reconstruct

6 vital areas to focus on early after ACL surgery
ACL rehabilitation, while surgical intervention can restore knee stability, the post-operative journ

Jumpers knee – Symptoms, risk factors & healing timeframe
Patellar tedninopathy, aka jumpers knee is a common and a pretty simple condition to diagnose if you
Leave a Reply