Graft rupture risk factors after ACL-Reconstruction
Delving into the complexities of ACL injuries, especially in athletes who have undergone reconstruction, reveals a puzzling reality—around 10% of those successfully returning to pre-injury activity levels face a second ACL injury. The grim prospect of graft rupture not only jeopardises function but also heightens the risk of early-onset knee osteoarthritis.
Surprisingly, the factors contributing to re-rupture remain poorly understood. This article will discuss the findings from Cronstrom and colleagues (2023) from the paper Return to Sports: A Risky Business? A Systematic Review with Meta-Analysis of Risk Factors for Graft Rupture Following ACL Reconstruction and give further explanations.
Let’s jump in!
7 key risk factors associated with ACL re-rupture
7 key factors emerged as risk factors for ACL re-rupture
- High activity level, especially with a Tegner score of ≥ 7 compared to < 7 at the primary injury (moderate quality evidence).
- Young age, with odds 2.6–3.5 times higher for those aged < 18–30 years compared to those ≥ 18–30 years (low to moderate quality evidence).
- Increased lateral tibial slope (very low quality evidence).
- Lower psychological readiness (very low quality evidence).
- Surgery within 12 months compared to surgery ≥ 12 months post-injury (moderate quality evidence).
- Returning to pre-injury activity level (moderate quality evidence).
- A family history of ACL injury (moderate quality evidence).
Join our newsletter and get break down of sports medicine research

- Higher age (moderate quality evidence).
- Female sex (low quality evidence).
- Better pre-reconstruction score on the Knee Injury and Osteoarthritis Outcome Score (KOOS) (low quality evidence).
- Accompanied cartilage injury (moderate quality evidence)
Factors that are NOT associated with re-rupture
- High BMI
- Smoking status
- Contact versus non-contact injury mechanism
- Medial tibial slope
- General joint laxity
- Pre-reconstruction KOOS score
- Timing of surgery (≥ 3 vs. < 3 months or ≥ 6 vs. < 6 months)
- Number of physical therapy visits
- Timing of return to sport (≥ 6 vs. < 6 months),
- Playing soccer compared with other sports
- Hop performance
- Quadriceps strength / hamstring strength
- Knee abduction after return to sport
A deeper look into the Risk factors
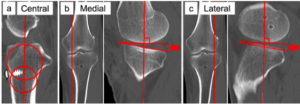
Understanding Tibial Slope and ACL Risk
Research indicates that a higher lateral tibial slope is associated with an elevated risk of graft rupture. This link is attributed to the potential impact on forward tibial movement and internal rotation during activities. This heightened movement may subsequently elevate the strain on the ACL. Notably, medial slope doesn’t seem to be a risk factor for ACL re-rupture.
Activity Levels Post-ACL Reconstruction
A pre-injury Tegner score of ≥ 7, indicating a high activity level, was associated with the highest odds of experiencing graft rupture.
Returning to the same activity level as pre-injury after ACL reconstruction was linked to nearly twice the odds of future graft rupture. It’s noteworthy that the timing of the return to sport (whether less than 6 months or 6 months or more) and the specific sport (football vs. other sports) did not show a significant association with graft rupture.
That being said, it’s important to not rush the process. Strength & conditioning coaches and physiotherapists should consider the demands of the sport when planning rehabilitation and return to sports protocols, emphasising a personalised approach that aligns with the persons pre-injury activity level and the nature of the sport.
The Tegner and Lyshome knee quastionnaires – Click here
ACL tears before 20
The review by Cronstorm demonstrated that being younger is indeed a risk factor for graft rupture.
In particular, young adults under 20 years old faced 3.53 times higher odds of experiencing a future graft rupture compared to their counterparts over 20 years old. This elevated risk among the younger demographic may be attributed, in part, to the ongoing anatomical and neuromuscular development during adolescence.
Moreover, athletes under 20 years old often engage in high-level sports and may return to sports without achieving optimal knee function, further heightening their susceptibility to graft rupture.
Genetic Influences on ACL Graft Rupture
The presence of a family history of ACL injury emerges as a significant factor influencing the risk of graft rupture, impacting both adults and younger individuals. People with parents or siblings who have experienced ACL injuries face an increased likelihood of graft rupture compared to those without such a family history.
This observed trend could be attributed to specific gene variations (polymorphisms) and/or the inheritance of anatomical, biomechanical, and neuromuscular factors that collectively influence the risk of ACL injury.

Joint Laxity and ACL Graft Rupture
While this review did not establish a direct connection between general joint laxity and the risk of graft rupture, a study by Hewett et al. (2009) offers intriguing observations. Specifically, the case of two fraternal female twins who both experienced ACL injuries highlighted increased joint laxity in conjunction with changes in joint biomechanics during movement. These alterations included increased knee abduction and decreased knee flexion, along with shifts in patterns of muscle activation.
These findings suggest a potential link between joint laxity and ACL injuries, indicating that the relationship might be complex and individualised. While general joint laxity may not universally predict graft rupture, the case of these twins emphasises the need for a more nuanced understanding of joint biomechanics and muscle activation patterns in specific individuals.
Timing of ACL Reconstruction: Balancing Risks and Rewards
The timing of ACL reconstruction (ACLR) emerges as a critical factor influencing the risk of graft rupture. Strikingly, individuals undergoing ACLR within 12 months after injury faced an 87% increased chance of experiencing graft rupture compared to those who opted for delayed surgery (12 months or more).
This finding prompts a nuanced exploration of patient characteristics and activity levels associated with different surgical timings. The elevated risk in the early reconstruction group suggests a potentially higher post-operative activity level, while those delaying surgery may exhibit lower pre-injury activity levels or have no desire to return to their normal sport participation. This lower activity level in the delayed group could contribute to reduced strain on the knee, lowering the risk of graft rupture.
Moreover, the delayed surgery group may include a subgroup known as ‘copers’—individuals capable of returning to sports with excellent knee stability post-ACLR. Studies indicate that copers have a higher chance of rehabilitation success and a lower graft rupture rate.
The systematic review & meta-analysis by Ferguson et al (2019) compared the outcomes of early knee surgery (within 3 weeks) versus delayed surgery. The Tegner activity scale showed a significant 0.39-point improvement in favor of early surgery, indicating better functional outcomes. However, no significant differences were found in patient-reported Lysholm scores or intra-operative findings of meniscal lesions. There was a trend towards significance for chondral lesions in the early surgery group. Overall, the studies were rated fair or good on the Downs and Black checklist, and none were excluded due to bias.
Gender Dynamics: A New Perspective
Challenging previous notions, the recent review presents a nuanced view on gender and its impact on the risk of ACL graft rupture, especially in the context of both adults, children and adolescents. Contrary to earlier research indicating a higher risk for females, the findings by Cronstorm and colleague reveal that females exhibit lower odds of experiencing graft rupture, aligning with a recent systematic review reporting a lower absolute risk in females compared to males.
Subgroup analyses focusing on adults alone revealed no notable sex difference in graft rupture likelihood. However, the odds for females decreased even further when examining individuals aged 19 and younger.
A noteworthy observation is that young males often return to sports earlier, more frequently, and at higher levels compared to their female counterparts. This behavioral difference in return to sport might clear up why young males demonstrate higher odds of graft rupture than young females.
Return to Sport After ACL Reconstruction
In this review, a specific subgroup analysis focusing on children and adolescents revealed that returning to sport did not significantly impact the risk of graft rupture. This observation challenges previous hypotheses and prompts a reconsideration of the relationship between returning to sport and graft rupture risk in teenagers.
However, it’s crucial to acknowledge that this subgroup analysis was based on a limited number of studies, introducing a potential limitation that could impact the overall interpretation of the results. The intricacies of return to sport after ACL reconstruction are undoubtedly complex, involving various factors such as rehabilitation protocols, individual patient characteristics, and the nature of the sport.
While these findings question the assumed link between return to sport and graft rupture in children and adolescents, further research with larger sample sizes and diverse populations is necessary for a broader understanding of the nuanced dynamics involved in resuming activity after ACLR.
Psychological Factors after ACL reconstruction
Lower psychological readiness, measured by the ACL Return to Sport scale 9-12 months post-surgery, was associated with a heightened risk of graft rupture. Additionally, kinesiophobia, or the fear of movement, emerged as a linked factor amplifying the risk.
These findings underscore the imperative of integrating psychological considerations into knee rehabilitation protocols, emphasising the need for targeted interventions to address mental readiness and lack of confidence.
Contrastingly, no significant association was identified between hop tests or muscle strength and graft rupture. However, a lower hamstring-to-quadriceps ratio upon return to sports was correlated with a higher risk of graft rupture, hilighting the importance of specific muscle balance in mitigating risk.
The limited number of studies available for analysis emphasises the critical need for further research, particularly in establishing consistent measures of psychological and sensorimotor factors as potential graft rupture risk factors. Future studies should prioritise standardised, responsive measures that can be influenced by training and intervention.

Non-risk factors for ACL re-rupture
Contrary to prior suggestions linking higher BMI and smoking to lower post-ACLR activity and function, the study by Cronstorm and colleagues discovered no direct association between BMI or smoking status and the risk of future graft rupture. This challenges previous assumptions.
Remarkably, when excluding one potentially biased study, having a BMI over 25 kg/m2 appeared to reduce the risk of graft rupture.
While knee movement patterns, muscle strength, hop performance, and self-reported knee confidence have been linked to second ACL injuries, data specifically on graft rupture as an independent factor were limited in our review. The scarcity of eligible articles examining objective and self-reported function as risk factors for graft rupture, partly due to the combination of graft rupture and chronic ACL injuries in pooled data, emphasises the gaps in our current understanding.
Clinical Strategies for ACLR Recovery in Young Athletes
For clinicians navigating the rehabilitation journey post-ACLR in patients, a holistic approach is paramount. Integration of psychological aspects into rehabilitation protocols is crucial. Facilitating open communication is vital by encouraging athletes to express concerns and worries, coupled with providing education and displaying compassion, nurtures trust and rapport. Objective psychological readiness assessments, such as ACL-RSI questionnaires, can serve as valuable tools in understanding the persons readiness for return to sport.
Early rehabilitation strategies must encompass neuromuscular control and reactive training. Particular attention should be dedicated to quadricep & hamstring training, however a full body approach is throughout the rehab process is crucial.
Source:
- Cronström, A., Tengman, E. and Häger, C.K., 2023. Return to sports: a risky business? A systematic review with meta-analysis of risk factors for graft rupture following ACL reconstruction. Sports medicine, 53(1), pp.91-110.
- Ferguson, D., Palmer, A., Khan, S., Oduoza, U. and Atkinson, H., 2019. Early or delayed anterior cruciate ligament reconstruction: is one superior? A systematic review and meta-analysis. European Journal of Orthopaedic Surgery & Traumatology, 29, pp.1277-1289.
- Hewett, T., Lynch, T., Ford, K., Gwin, R., Heidt, R. and Myer, G., 2009. Multiple risk factors related to familial predisposition to anterior cruciate ligament injury: fraternal twin sisters with ipsilateral ACL ruptures. British journal of sports medicine.
You May Also Like

Diagnose & treat jumpers knee effectively
This article provides essential insights in the world of patellar tendinopathy. It encompasses asses

Jumpers knee – Symptoms, risk factors & healing timeframe
Patellar tedninopathy, aka jumpers knee is a common and a pretty simple condition to diagnose if you
Iliotibial band: What is the function and how to manage discomfort?
The iliotibial band (ITB) stands as a resilient and fibrous fascial tissue, stretching from the ilia
Leave a Reply