
Calf strains – How common are they?
Are you a physiotherapy student looking to expand your knowledge on calf muscle strain? If so, you’ve come to the right place. Calf strain is a common injury that can occur in both athletes and non-athletes alike. It is characterised by pain at the posterior aspect of the leg and can affect either the gastrocnemius or soleus muscle, or in rare cases, both. It is important to distinguish which muscle is affected, as the treatment protocols can vary significantly.
As a physiotherapy student, understanding the underlying causes, anatomy and risk factors for developing calf strain is essential. Not only will it help you provide effective care for your patients, but it will also strengthen your knowledge base and enhance your professional development.
In this blog, we will delve deeper into the world of calf muscle strain, exploring everything from its causes and symptoms to the timeframe of healing. By the end, you will have a comprehensive understanding of this common injury and be better equipped to help your patients recover quickly and safely.
Let’s get started
Check out out article about comprehensive calf assessment & treatment – Learn More
5 key takeaways
- Calf injuries involve pain in the mid-leg due to increased activity, impact, or overuse, affecting either the gastrocnemius or soleus muscles.
- Athletes aged 22 to 28, primarily men, are most susceptible to calf injuries, with recurrence in 19% to 31% of cases.
- The calf muscles, gastrocnemius, and soleus, play a crucial role in foot movement and stability during activities like running.
- Gastrocnemius injuries result from sudden ballistic foot movements, while soleus injuries often stem from repetitive dorsiflexion during uphill running.
- Calf strains are common in sports involving sprinting and are more prevalent in older athletes, with varying symptoms and healing times based on severity
What is it?
It’s considered to be pain at the posterior aspect of the mid leg due to sudden increase in activity, impact or overuse. The strain can be either to the gastrocnemius muscle or the soleus muscle

Facts
- Calf injury is most prevalent among athletes 22 to 28 years of age, more frequently affects men
- Presents as a recurrent injury in approximately 19% to 31% of cases.
Anatomy
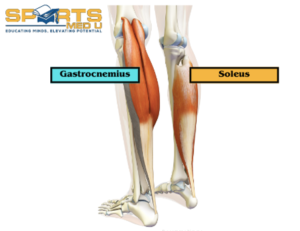
In overview, the gastrocnemius and soleus muscles originate from the posterior aspect of the leg and insert into the achilles tendon. They work together to plantarflex the foot and provide power and stability during activities such as walking, running, and jumping.
Gastrocnemius
Origin:
It’s a large, two-headed muscle. The medial head originates from the posterior surface of the femoral condyle, which is the rounded end of the femur bone in the thigh. The lateral head originates from the lateral condyle of the femur
Insertion:
The two heads of the gastrocnemius muscle merge into a single belly that inserts into the calcaneus bone via the Achilles tendon. This insertion point is located on the heel bone (calcaneus) and is known as the calcaneal tuberosity
Function:
The main function of the gastrocnemius muscle is to plantarflex the foot as well as assisting to flex the knee. When you stand on tiptoes or push off the ground while walking or running, the gastrocnemius muscle contracts, causing the ankle joint to extend and the heel to rise. It is an important muscle for walking, running, and jumping, as well as for maintaining posture while standing.
Soleus
Origin:
The soleus muscle originates from the head and shaft of the fibula bone, as well as the posterior surface of the tibia bone.
Insertion:
The muscle fibres then merge into a single belly that inserts into the calcaneus bone via the Achilles tendon, at the same point as the gastrocnemius muscle.
Function:
The main function of the soleus muscle is to plantarflex the foot, just like the gastrocnemius muscle. However, unlike the gastrocnemius, the soleus muscle is not involved in flexing the knee joint as it does not cross it. It’s primarily responsible for maintaining posture, especially when standing or walking slowly. It is also involved in helping to stabilize the ankle joint during weight-bearing activities.
Mechanism of injury
Gastrocnemius:
Classic mechanism of a gastrocnemius tear involves knee extension with sudden ballistic foot movement from dorsiflexion to plantar flexion. During sudden increase in tension the muscle gets maximally stretched, leading to an abrupt strain/rupture, most commonly in the medial head. The medial head is more vulnerable to injury than the lateral head due to its longer and narrower shape and smaller cross-sectional area.
Soleus:
Soleus muscle strain is an overuse condition that can occur because of repetitive, passive dorsiflexion of the foot with the knee bent. This can lead to strain or tearing of the soleus muscle fibres and is commonly observed in athletes who engage in activities that require repetitive uphill and/or long-distance running. Runners, in particular, may be more susceptible to developing soleus muscle strain due to the posture required during uphill running. The angle of incline can increase the strain on the soleus muscle as it works to maintain stability and control during each stride. This can result in fatigue, weakness, and eventual strain or tearing of the muscle fibres.

Frequency/Pattern of injury
The exact epidemiology of calf strains is not well-defined, but studies have shown that calf strains are more common in sports that involve sprinting, such as soccer, basketball, and track and field as well as long distance running. Calf strains can occur in athletes of all ages and genders, but they are more common in older athletes, possibly due to decreased muscle flexibility and strength with age
Symptoms & Clinical presentation
Symptoms and clinical presentation will characteristically differ dependent on what muscles of the calf complex are affected.
Here are key things to understand when diagnosing calf strains.
- Gastrocnemius strain is associated with high intensity running, acceleration, and deceleration activities – Gastro is dense in fast-twitch muscle fibres adapted for rapid contraction (Type 2 A and B)
- Acute strain of the gastrocnemius can present with an audible pop.
- This then is followed by dull to severe pain and swelling in the posterior lower limb within 24 hours
- The pain can be latent at the time of the injury, manifesting only after the person tries to stand, walk, or plantar flex the foot.
- Soleus strain is more likely to occur during steady-state running activities – Soleus is dense in slow-twitch muscle fibres adapted for postural control (Type 1)
- Client may complain of muscle tension and tightness,
- Pain may gradually development over the course of days to week
- Swelling is minimal and over calf functional ability is affected mildly
Clinical course
The clinical course of calf strain can vary depending on the severity of the injury. In general, mild strains may take several days to a week to resolve, while more severe strains may take several weeks or even months to fully heal.
Muscle healing time frames are:
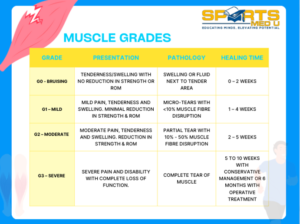
Imaging
Imaging for calf muscle strains is not often used in a clinical setting as it can be diagnosed with subjective and objective testing alone, However in cases where the diagnosis is uncertain or there is suspicion of a more severe injury imaging can be a very helpful tool to guide diagnosis and treatment.
The frequency of use may vary depending on the healthcare provider’s experience and training, the availability of imaging facilities, and the specific clinical scenario.
For example, in a primary care setting, imaging may not be routinely ordered for a mild to moderate calf muscle strain. In a sports medicine or orthopaedic setting on the other hand, imaging may be used more frequently to help guide treatment and assess the extent of the injury.
Ultimately, the decision to use imaging for calf muscle strains will depend on the healthcare provider’s judgment and the specific circumstances of the patient’s injury.
- Ultrasound is often the preferred imaging modality as it is non-invasive, readily available, and cost-effective. It can help identify muscle tears, fluid accumulation, and tissue damage. It can also be used to guide therapeutic injections.
- MRI is a more advanced imaging technique that can provide a detailed view of the soft tissues, such as muscles, tendons, and ligaments. It can help identify the exact location and extent of the injury and is particularly useful in cases of severe or complicated calf muscle strains. It also helps to detect intramuscular fluid collection, which is associated with delayed return to play
Surgery
Surgery is not typically used to treat isolated calf muscle injuries, as most strains can be managed conservatively, along with appropriate rehabilitation exercises. However, in cases where the muscle strain is severe or complicated by other injuries, surgery may be necessary.
For example, if a calf muscle strain is associated with a complete tear of the Achilles tendon or a fracture of the tibia bone, surgical intervention may be required to repair the damage and restore normal function. In general, surgical intervention for calf muscle strains is rare and reserved for cases where non-surgical management has failed or is not appropriate
Risk factors for sustaining a calf strain
The risk factors for a calf muscle strain are mostly generic to all muscle injuries. Key areas to be mindful of are:
Age
- A possible explanation is that age-related tissue changes involve progressive declines in skeletal muscle quality and function.
- The consequences of which include neuromuscular maladaptation’s that restrict muscle force and rate of contraction.
History of calf strain or other lower limb injuries
- Prior injuries in the calf, hamstrings, quadriceps, adductors, and knee have been identified as risk factors for a subsequent calf injury due to over compensation of other muscles
Summary of article:
Calf strain can be either to the gastrocnemius muscle or the soleus muscle. The gastrocnemius muscle is a large, two-headed muscle, while the soleus muscle originates from the head and shaft of the fibula bone, as well as the posterior surface of the tibia bone. The gastrocnemius muscle contracts during activities such as standing on tiptoes, running, and jumping, while the soleus muscle is primarily responsible for maintaining posture.
The classic mechanism of a gastrocnemius tear involves sudden ballistic foot movement from dorsiflexion to plantar flexion, while soleus muscle strain is an overuse condition that can occur due to repetitive, passive dorsiflexion of the foot with the knee bent. Calf strains are more common in sports that involve sprinting, such as soccer, basketball, and track and field, as well as long-distance running.
The symptoms and clinical presentation of calf strains differ depending on what muscles of the calf complex are affected. The clinical course of calf strain can vary depending on the severity of the injury. Mild strains may take several days to a week to resolve, while more severe strains may take several weeks or even months to fully heal.
Source
- Baoge, L., Van Den Steen, E.L.K.E., Rimbaut, S., Philips, N., Witvrouw, E., Almqvist, K.F., Vanderstraeten, G. and Vanden Bossche, L.C., 2012. Treatment of skeletal muscle injury: a review. International Scholarly Research Notices, 2012.
- Green, B. and Pizzari, T., 2017. Calf muscle strain injuries in sport: a systematic review of risk factors for injury. British journal of sports medicine, 51(16), pp.1189-1194.
- Meek, W.M., Kucharik, M.P., Eberlin, C.T., Naessig, S.A., Rudisill, S.S. and Martin, S.D., 2022. Calf Strain in Athletes. JBJS reviews, 10(3), p.e21
- Pierpoint, L.A., Williams, C.M., Fields, S.K. and Comstock, R.D., 2016. Epidemiology of injuries in United States high school track and field: 2008-2009 through 2013-2014. The American journal of sports medicine, 44(6), pp.1463-1468.
You May Also Like

Dynamic stretching – Does it reduce risk of injury?
In the pursuit of peak athletic performance, the role of stretching, both static and dynamic, has be

Frozen Shoulder: Assessing & Managing
As a clinician, encountering perplexing cases of persistent shoulder pain is not uncommon. Enter the

Achilles Tendinopathy: Assessment & Treatment
Are you struggling with Achilles tendinopathy and looking for effective solutions? Look no further!
Leave a Reply